Procedure Overview
What Is Hip Resurfacing?
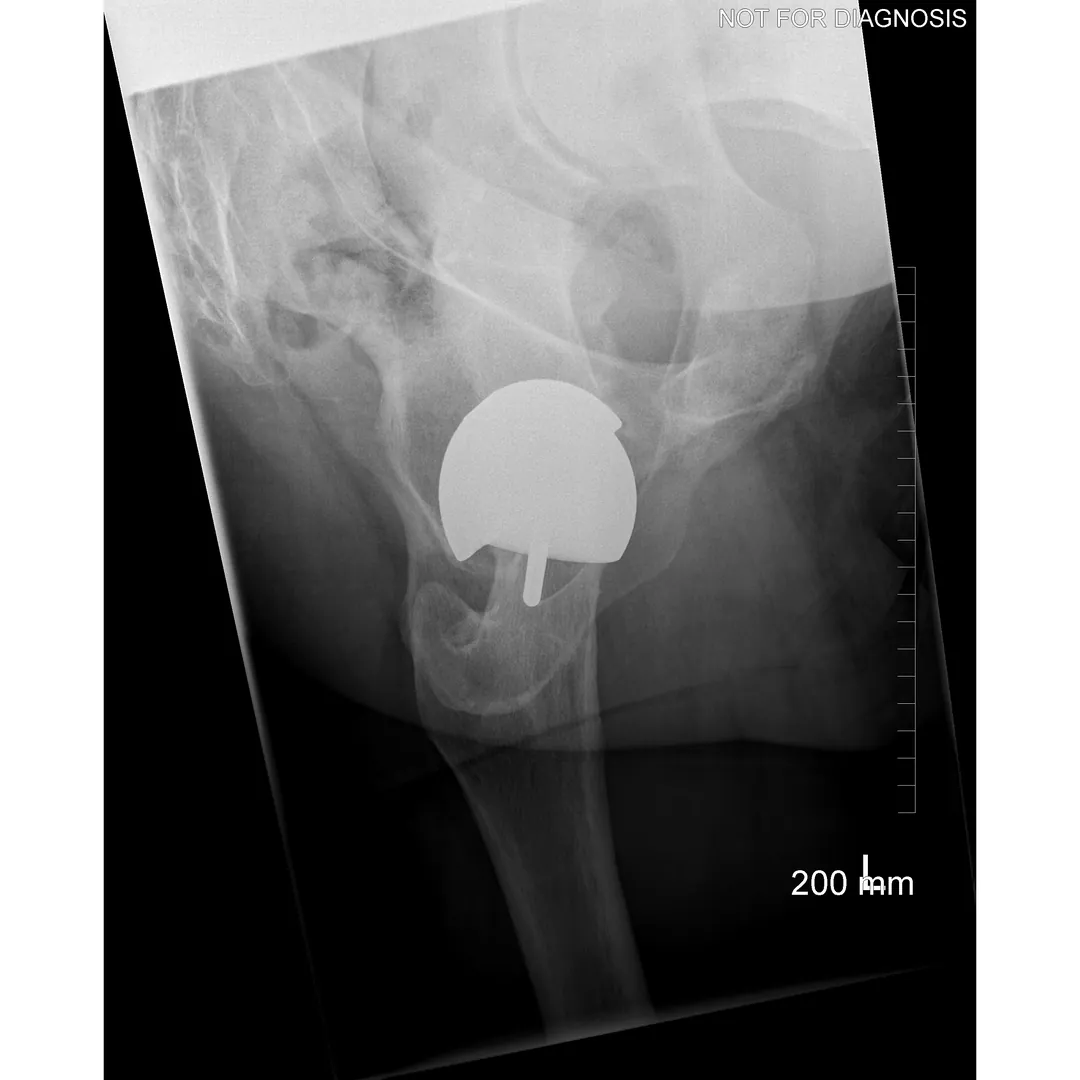
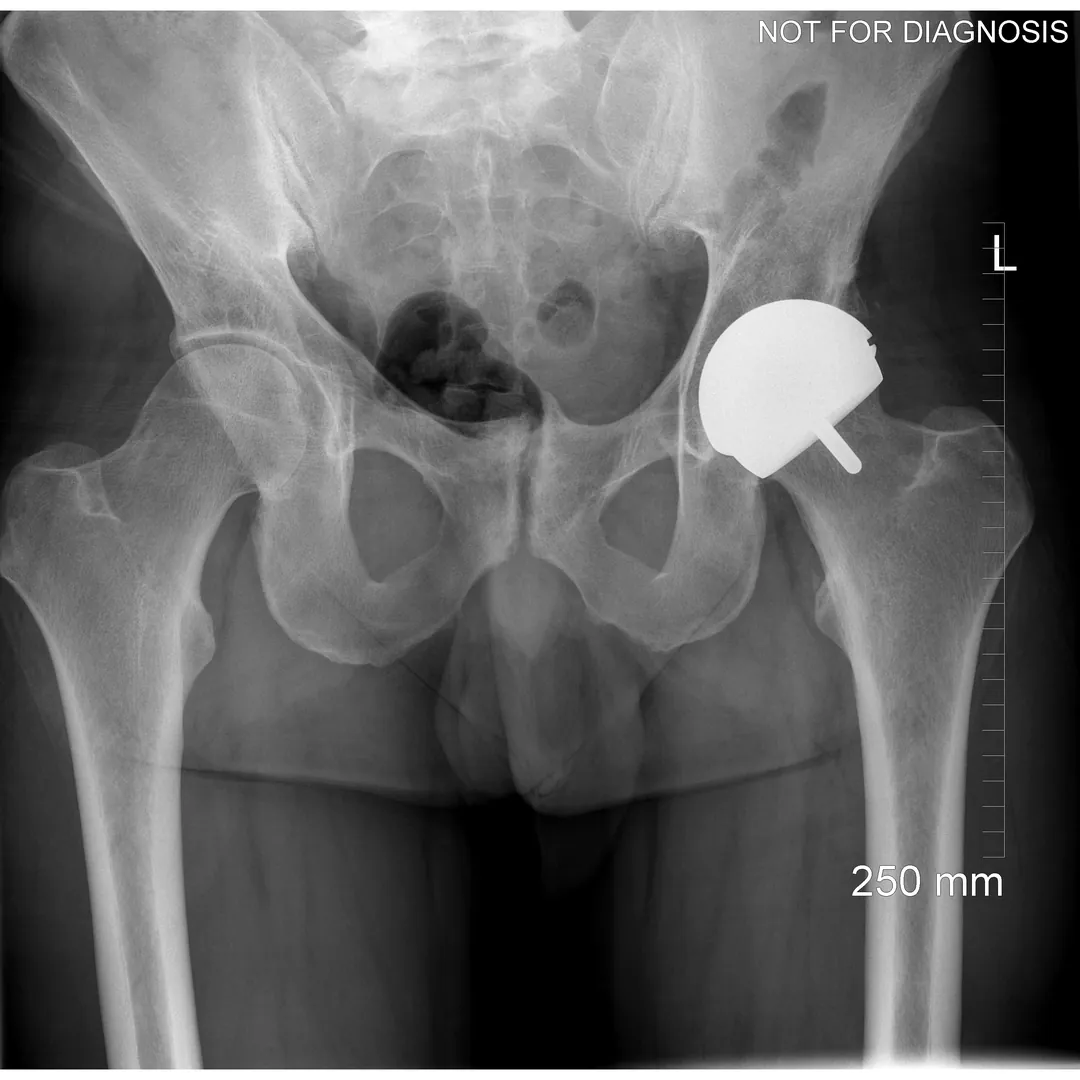
Hip resurfacing is a type of hip surgery used to treat hip arthritis, most commonly in younger and more active patients. Unlike a total hip replacement, hip resurfacing preserves more of your natural thigh bone. Instead of removing the entire femoral head (ball at the top of the thigh bone), the damaged surface is trimmed and covered with a smooth metal cap. The hip’s socket on the pelvis is also fitted with a metal cup.
The goal of hip resurfacing is to relieve pain, restore function, and allow a return to an active lifestyle while preserving bone for potential future surgery.
Who Is (and Is Not) a Good Candidate for Hip Resurfacing
Hip resurfacing can be an excellent option for carefully selected patients, but it is not suitable for everyone.
Careful assessment is essential.
You May Be a Good Candidate If You:
- Have severe hip pain due to arthritis that limits daily activities
- Are younger and physically active
- Have good bone quality and strong femoral neck bone
- Have a larger femoral head size
- Have minimal deformity of the hip joint
- Have not improved with non-surgical treatments (medications, injections, physiotherapy)
- Are Male (Hip Resurfacing of Metal-on-Metal bearings are not offered in Females, due to increased failure rates). Females may be candidates for Ceramic-on-
Ceramic Hip Resurfacings: (please read below)
- Hip Resurfacing May Be Less Suitable If You:
- Have poor bone quality or osteoporosis
- Have a small femoral head size
- Have advanced deformity or collapse of the femoral head
- Have inflammatory arthritis (such as rheumatoid arthritis)
- Have significant kidney disease
- Have known or suspected metal sensitivity
- Are planning pregnancy (in some cases, due to metal ion considerations)
Important Individual Factors:
- Age alone does not determine suitability, as bone quality and anatomy are critical
Women may be not suitable candidates for metal-on-metal hip resurfacing due to bone size, quality, and bone angles.
Final decision-making should involve a detailed discussion with your surgeon about risks, benefits, and alternatives
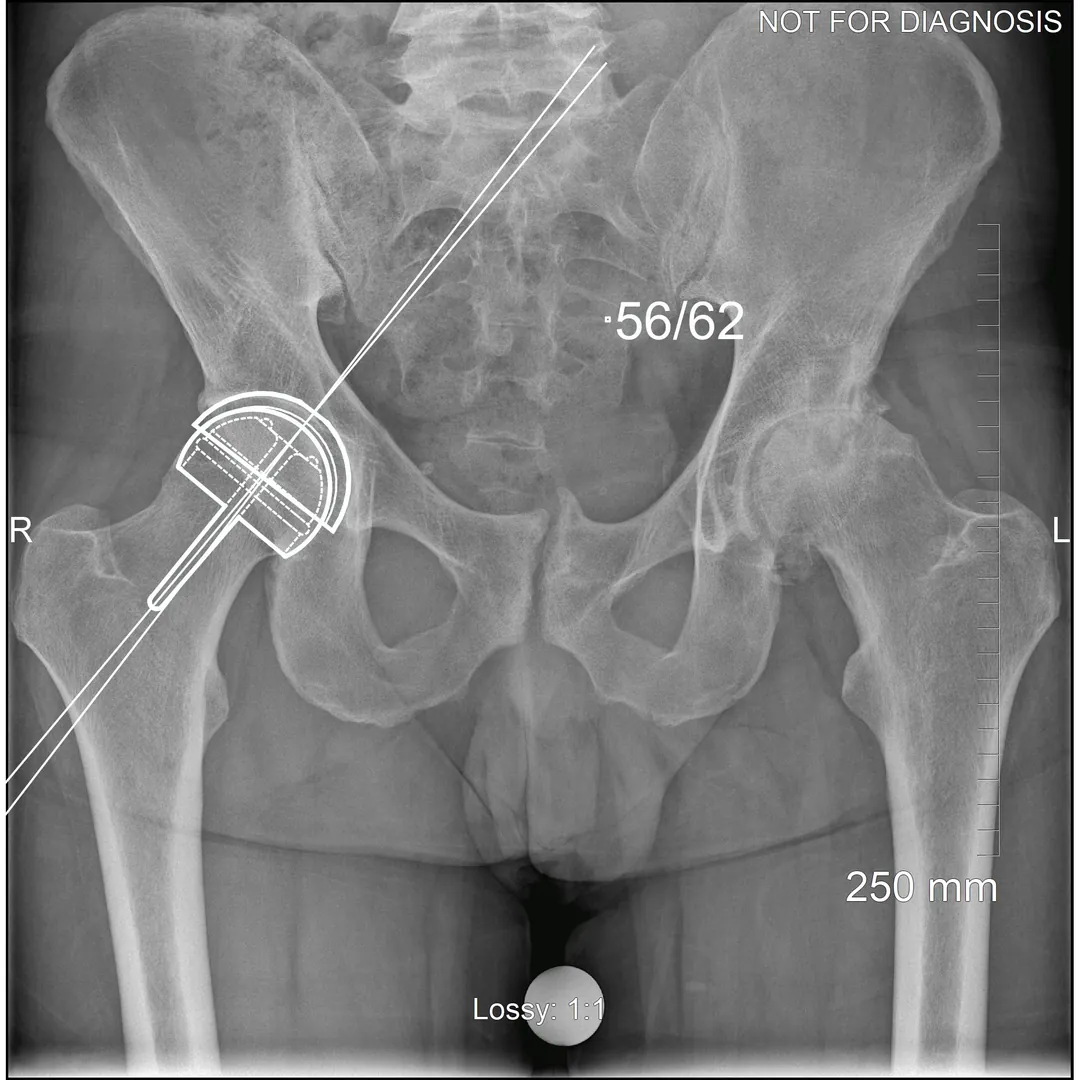
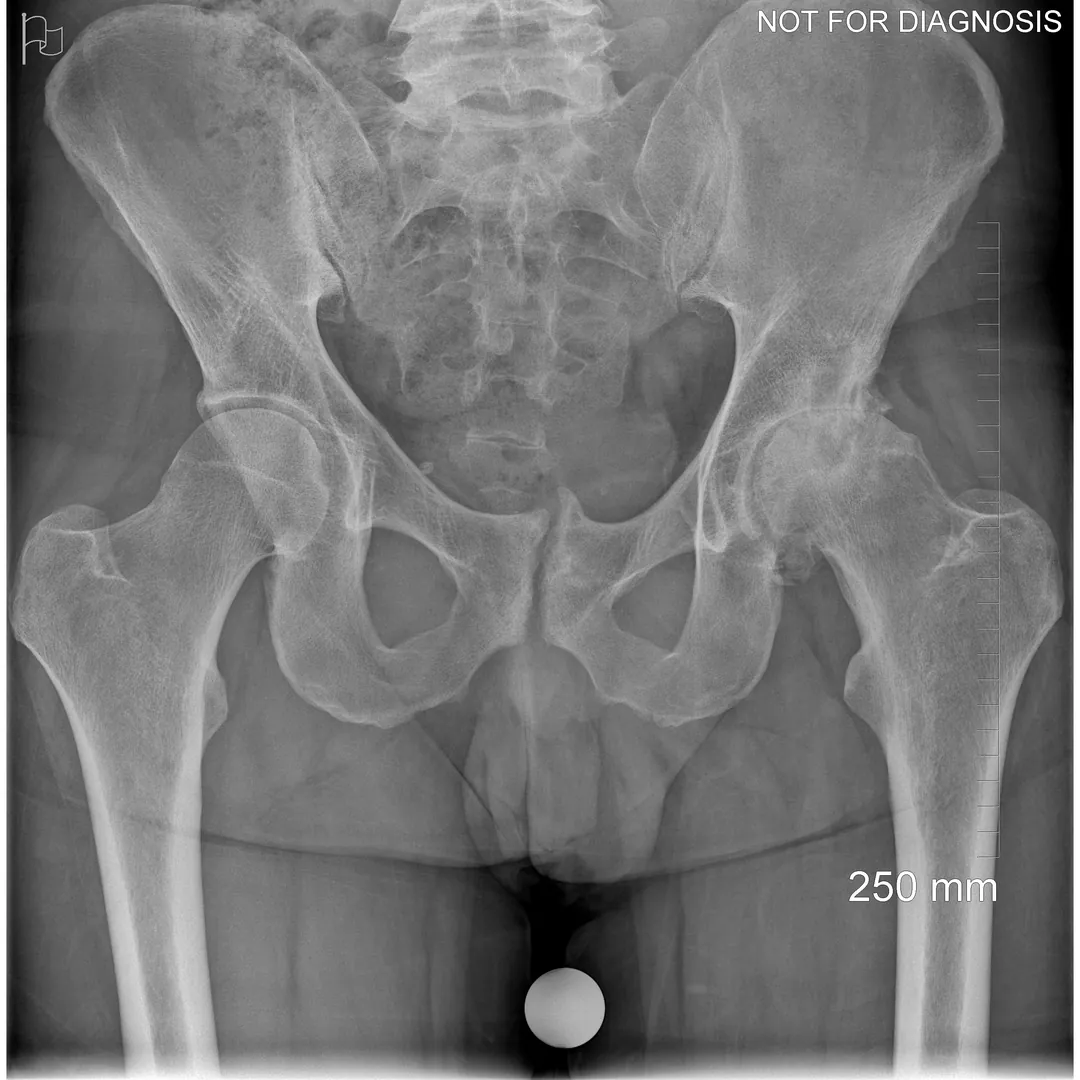
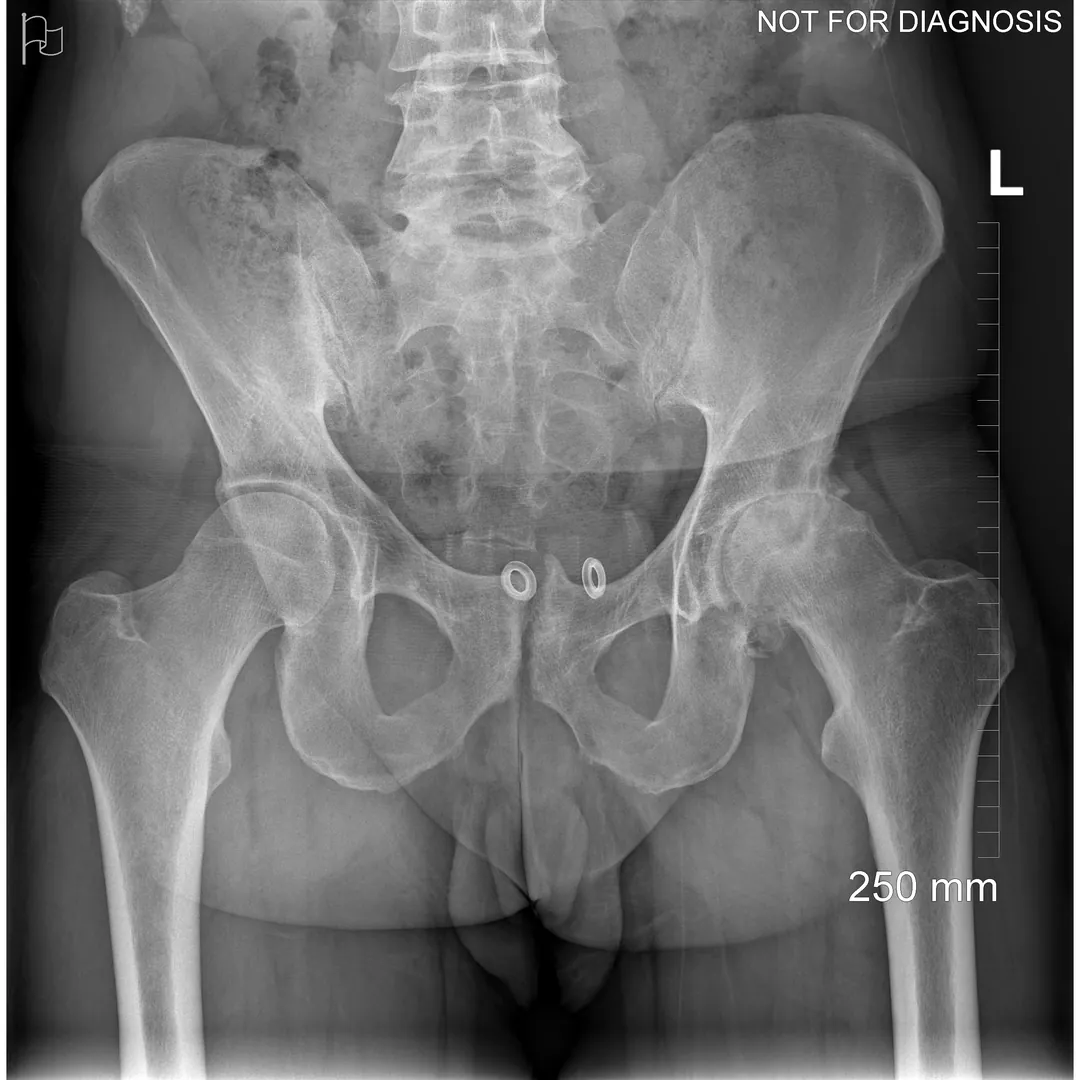
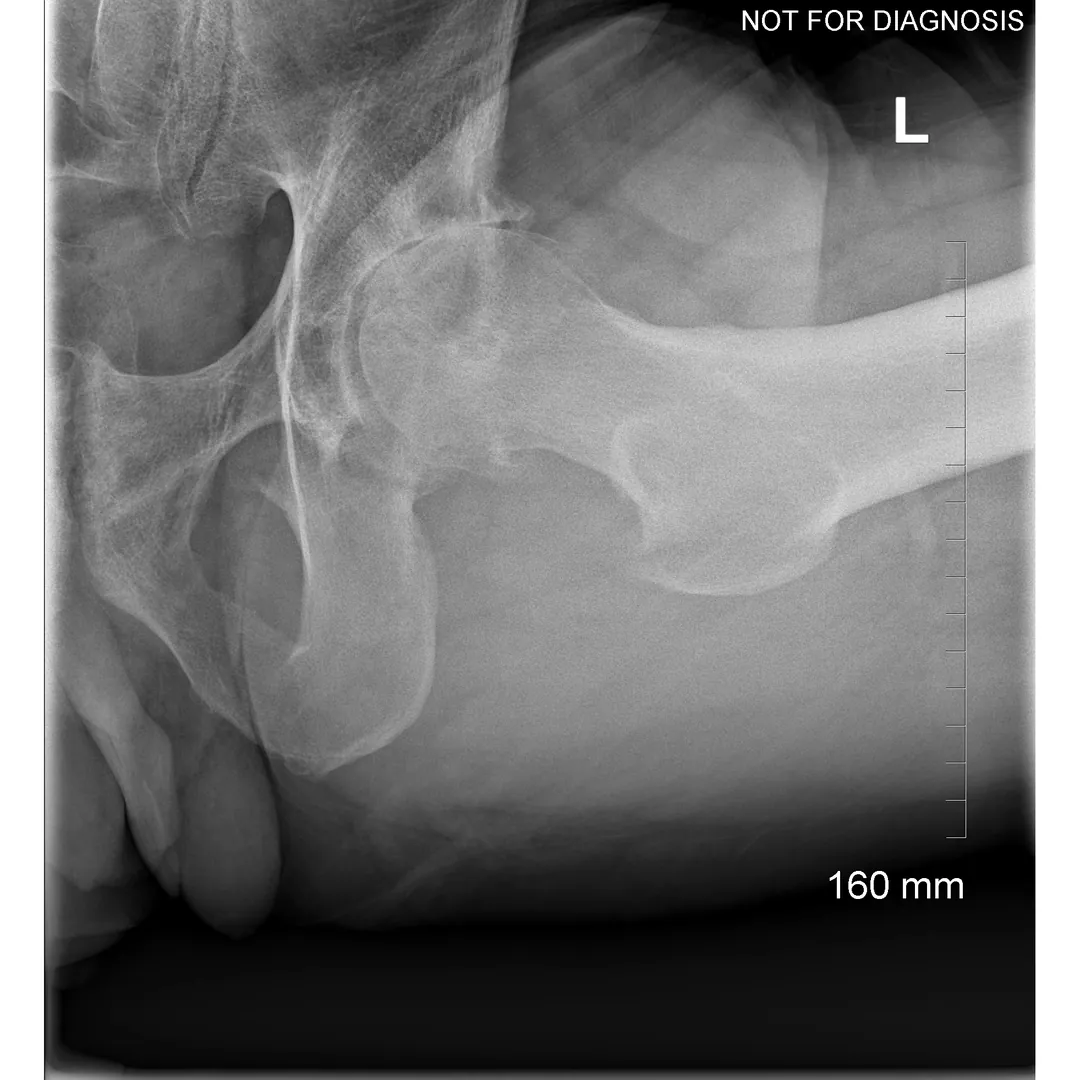
Dr Grammatopoulos will review your X-rays and other imaging carefully to determine whether hip resurfacing is an appropriate option for you.
Clinical Outcomes & Patient Safety
Key Benefits
- Preserves more natural bone compared to total hip replacement
- Lower risk of hip dislocation due to larger ball size
- May feel more natural during movement
- Allows higher activity levels in selected patients
- Easier conversion to total hip replacement if needed in the future
Risks & Considerations
- Infection
- Blood clots
- Nerve or blood vessel injury
- Fracture of the femoral neck
- Implant loosening or failure
- Ongoing pain or stiffness
- Hip resurfacing may also involve bearing-surface–specific risks (depending on implant type), especially with metal-on-metal implants.
Decision Aid: Hip Resurfacing vs Total Hip Replacement
This section is designed to help you compare hip resurfacing and total hip replacement (THA). It does not replace a discussion with your surgeon, who will recommend the safest and most appropriate option for your situation.
Why do metal ions matter?
With MoM bearings, very small metal particles can be released with movement. In some patients, this can lead to:- Local inflammation around the hip
- Fluid collections or soft tissue masses
- Bone or muscle damage that can make future revision surgery more complex
- Monitoring and Follow-Up
- Regular clinical follow-up
- Periodic blood tests for cobalt and chromium levels (if recommended)
- maging such as ultrasound or MRI (often with metal artifact reduction techniques) if symptoms develop
- You are a younger, active person with good bone quality
- Your hip anatomy is suitable (often a larger femoral head size)
- You want to preserve bone for potential future surgery
- You understand the need for long-term follow-up (especially with metal-on-metal implants)
Total Hip Replacement (THA) may be a better fit if:
- You have a broader range of arthritis severity or anatomy
- You have lower bone quality or a smaller femoral head size
- You prefer an implant option with many bearing choices (often non–metal-on-metal)
- You want the most widely performed procedure with extensive long-term outcome data
Risks of Metal-on-Metal Hip Resurfacing:
What Patients Should Know: When to Seek Review Contact your surgeon if you develop:- New or worsening hip pain
- Swelling, clicking, or instability
- Reduced walking tolerance
- Unexplained symptoms you are concerned about (your care team can advise what is relevant)
Surgical Approaches
Hip Resurfacing vs. Total Hip Replacement (THA)
Hip Resurfacing
- Preserves more natural bone (the femoral head is capped rather than replaced)
- Uses a larger ball size, which may reduce the risk of dislocation
- Often considered for younger, active patients with good bone quality
- If needed, it can usually be revised to a total hip replacement
Total Hip Replacement (THA)
- Removes the femoral head and replaces it with a stem and ball
- Replaces the socket with a cup and liner (many bearing options exist)
- Suitable for a wider range of patients, including those with more advanced arthritis
- Excellent pain relief and predictable outcomes for most patients
Newer Bearing Options: Ceramic-on-Ceramic Hip Resurfacing
- Potential Advantages (Theoretical and Early Evidence)
- Minimal metal ion release from the bearing surface
- Low wear characteristics of ceramic
- Ceramic materials can be more brittle than metal, and component design and surgical technique are important
- Availability may be limited and not all centres offer these implants
- Long-term outcomes and durability data may be more limited compared with established total hip replacement bearings
- Your surgeon can discuss whether a newer bearing option is appropriate and available for you.
Step 2: Compare key trade-offs
| Feature | Hip Resurfacing | Total Hip Replacement (THA) |
|---|---|---|
| Main goal | Preserve your natural bone and hip mechanics | Replace the arthritic joint reliably |
| Bone preserved | More (femoral head stays) | Less (femoral head removed) |
| Dislocation risk | Often lower (larger ball) | Low (varies by approach/implant) |
| Unique risks | Femoral neck fracture; metal ion issues (MoM) | Dislocation (varies); implant wear/loosening over time |
| Follow-up needs | May need periodic monitoring (symptoms, metal ions, imaging) | Routine follow-up; monitoring depends on implant and symptoms |
| If future surgery needed | Often conversion to THA | Revision THA |
| Best evidence base | Strong in selected patients; not for everyone | Very strong across broad patient groups |
Step 3: Questions to ask your surgeon
- Am I a candidate for hip resurfacing based on my X-rays and bone quality?
- What implant type and bearing surface would be used, and why?
- What are the expected recovery milestones for my situation?
- What activities will you recommend after surgery?
- What follow-up schedule do you recommend, and will I need blood tests or imaging?
Procedure Steps
- Total hip replacement usually takes 1–2 hours
- It is performed under general or spinal anesthesia
- The surgeon removes the damaged bone and cartilage and inserts the artificial joint
- The incision is then closed with sutures or staples
Preparing for Surgery
Good preparation before surgery can improve recovery and reduce complications. Your healthcare team will guide you, but general recommendations include:
Medical Preparation
- Attending a preoperative assessment clinic to review your overall health. This may require blood tests, X-rays, and heart tests.
- Reviewing medications with your healthcare provider, as some may need to be stopped before surgery.
- Managing existing conditions (such as diabetes, anemia, high blood pressure, or heart disease) as well as possible
- Treating existing infections (including dental, skin, or urinary infections) before surgery
Lifestyle Preparation
- Stop smoking, ideally several weeks before surgery, as smoking can delay healing and increase risk of complications
- Maintain a healthy diet rich in protein, vitamins, and minerals to support healing
- If advised, try to lose excess weight to reduce stress on the new joint
- Begin preoperative exercises ("prehabilitation") to strengthen hip and leg muscles and improve flexibility
Plan Ahead
- Arrange time off work and discuss return-to-work plans with your healthcare provider
- Organize help at home for the first few weeks after surgery
- Plan transportation to and from the hospital on the day of surgery and for follow-up appointments. You will not be able to drive initially.
- Prepare questions and concerns to discuss with your surgical team
What to Expect After Surgery
 Recovery In Hospital
Recovery In Hospital
- Most patients have a hospital stay of 1–3 days, depending on recovery and overall health
- Pain will be managed with medications
- You will begin walking with physiotherapy assistance, often the day after surgery
- Blood-thinning medications may be prescribed to reduce clot risk
- Nurses and therapists will teach you how to move safely, get in and out of bed, dress, and use the bathroom
 Recovery At Home
Recovery At Home
Preparing your home before surgery can help make your recovery smoother and more comfortable.
Upon your return home, you can expect to:
- Require walking aids (walker or crutches) for several weeks
- Continue with prescribed physiotherapy
- Experience pain, swelling and stiffness initially
- Gradually return to activities is encouraged
Return to Work, Driving & Sports
 Return to Work
Return to Work
- Sedentary or desk-based work: Often 4–6 weeks after surgery
- Light physical work: Usually 6–8 weeks
- Heavy manual labour: 8–12 weeks or longer and should be discussed with your surgeon
 Driving
Driving
- You are no longer taking narcotic pain medication
- You can safely control the vehicle and perform an emergency stop
- Your surgeon confirms it is safe
 Sports
Sports
- Walking
- Swimming
- Cycling
- Lower-impact fitness programs
Some surgeons may allow return to higher-impact activities in carefully selected patients. This should be discussed individually.
Implant Longevity & Dental Advisory
 Implant Longevity
Implant Longevity
 Dental & Antibiotics
Dental & Antibiotics
- Patients should not be exposed to the adverse effects of antibiotics when there is no evidence that such prophylaxis is of any benefit.
- Routine antibiotic prophylaxis is not indicated for dental patients with total joint replacements, nor for patients with orthopedic pins, plates and screws.
- Patients should be in optimal oral health prior to having total joint replacement and should maintain good oral hygiene and oral health following surgery. Orofacial infections in all patients, including those with total joint prostheses, should be treated to eliminate the source of infection and prevent its spread.
- Have a weakened immune system
- Have poorly controlled diabetes
- Have had previous joint infections
- Are undergoing invasive dental procedures involving significant gum manipulation
Frequently Asked Questions
Is hip resurfacing the same as a total hip replacement?
No. Hip resurfacing preserves more bone and uses different implants, but both aim to relieve pain and improve function.
Can hip resurfacing be revised to a hip replacement?
Yes. If needed, hip resurfacing can be converted to a total hip replacement.
Is hip resurfacing suitable for women?
Hip resurfacing may be less suitable for some women due to bone size and quality. Your surgeon will assess this individually.